The past few months have been a whirlwind of attending and speaking at medical conferences and staying up to date on new research and publications. Today’s Substack will be a review of where I have been and what I have learned since the start of 2026! Let’s just say… the sky is opalite.
Harvard Women’s Health & Menopause Conference
It was a true honor to be asked to present at the Harvard Women’s Health & Menopause Conference. On the heels of my presentation at The Young Survival Coalition, and with my YSC fan in hand ( more about that here) , I was proud to present to almost 2000 clinicians on what I am most passionate about: the unique challenges of young breast cancer and how to manage menopause after cancer. My talks were followed by an expert panel with Drs. Comander, Isakoff and Bluming, where we fielded challenging questions.
This year marks 25 years from my diagnosis at age 28, and being invited to speak at Harvard and be on a panel with these incredible physicians was my true silver linings playbook!
Guess what? We all agreed on everything! Yes! Three medical breast oncologists and an OBGYN and we all agree that:
Breast cancer survivors need far more support and attention on the collateral damage of induced premature menopause and prolonged hormone deprivation.
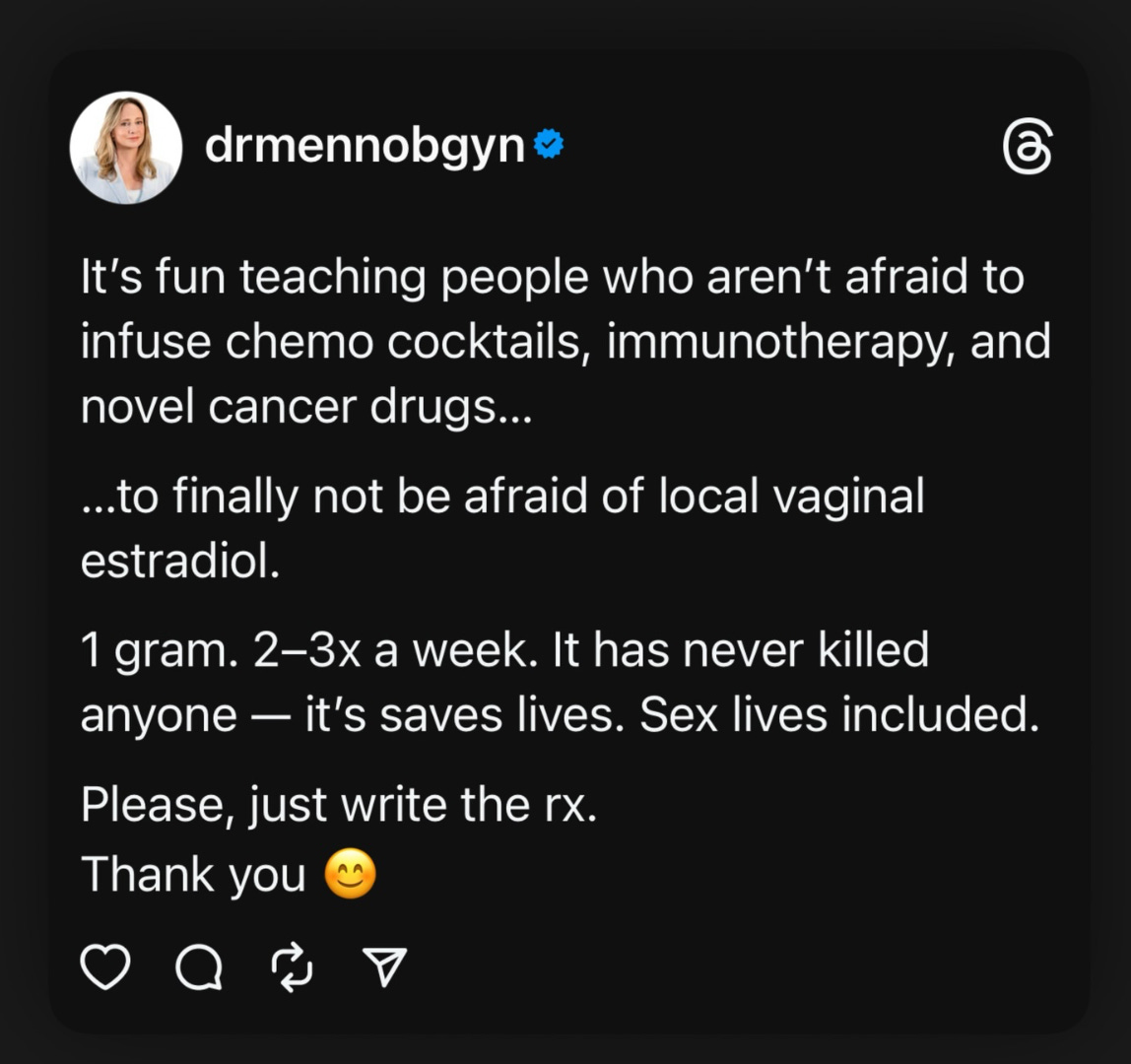
VAGINAL HORMONES ARE SAFE FOR ALL WOMEN WITH BREAST CANCER. Yes, even those on adjuvant endocrine therapy.
Systemic hormone use after breast cancer should not be absolutely prohibited, but rather the decision to use should be individualized based on the specific type of breast cancer, risk of recurrence, symptom burden, and ultimately the health goals of the patient.
From Harvard, I flew to Cleveland for the National Consortium of Breast Center 35th Annual Interdisciplinary Breast Cancer Conference, where I had two presentations: “Menopause Management and Breast Cancer” and “Managing GSM and Sexual Dysfunction”. It was an honor to speak in the presence of my friend and mentor, the incredible Dr. Holly Pederson, who was the director of Medical Breast Services at the Cleveland Clinic and an expert in managing women at high risk.
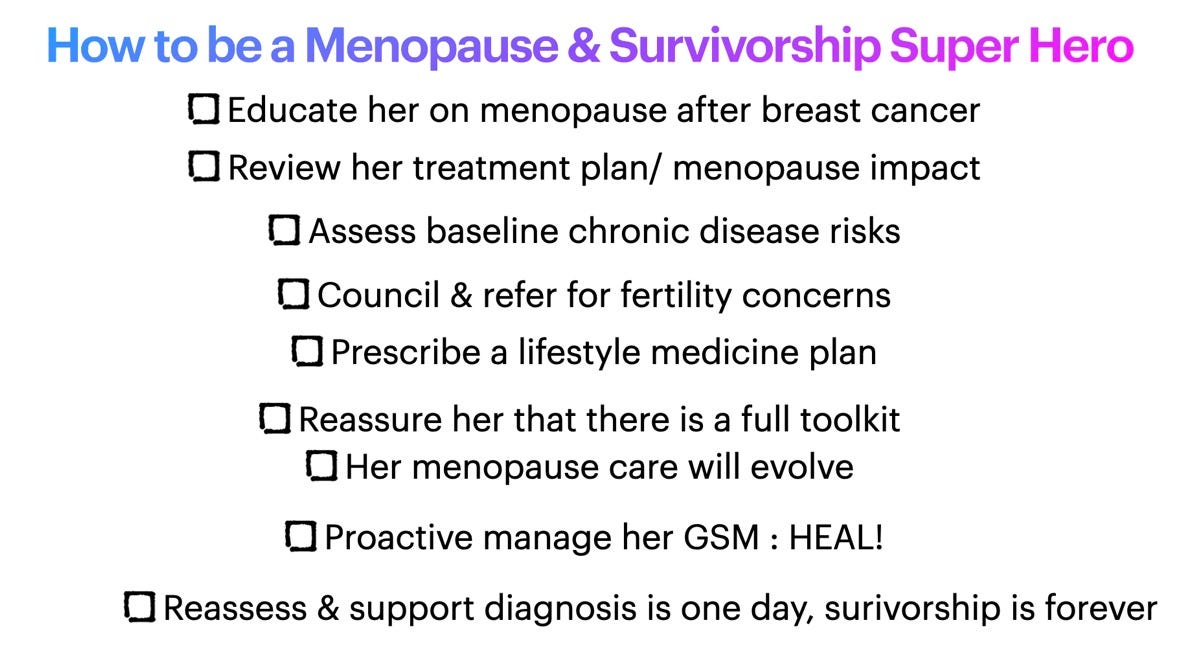
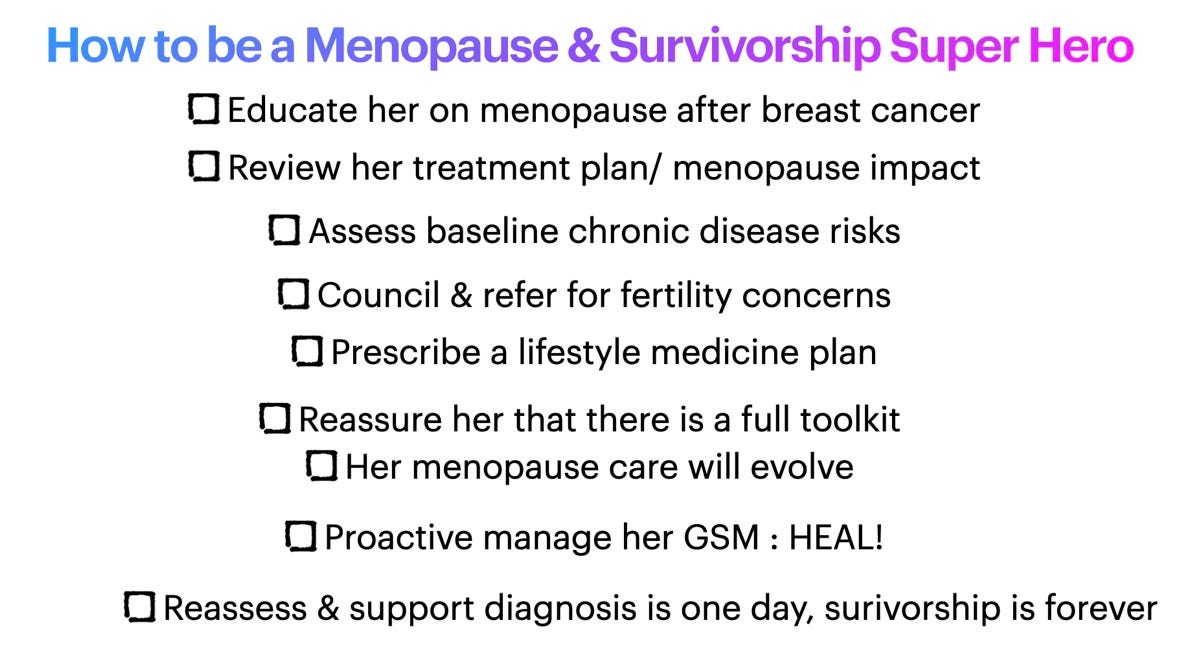
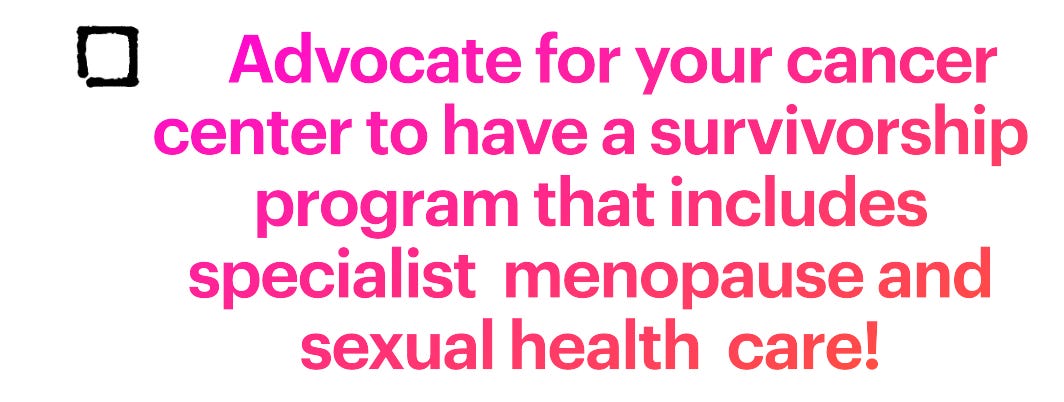
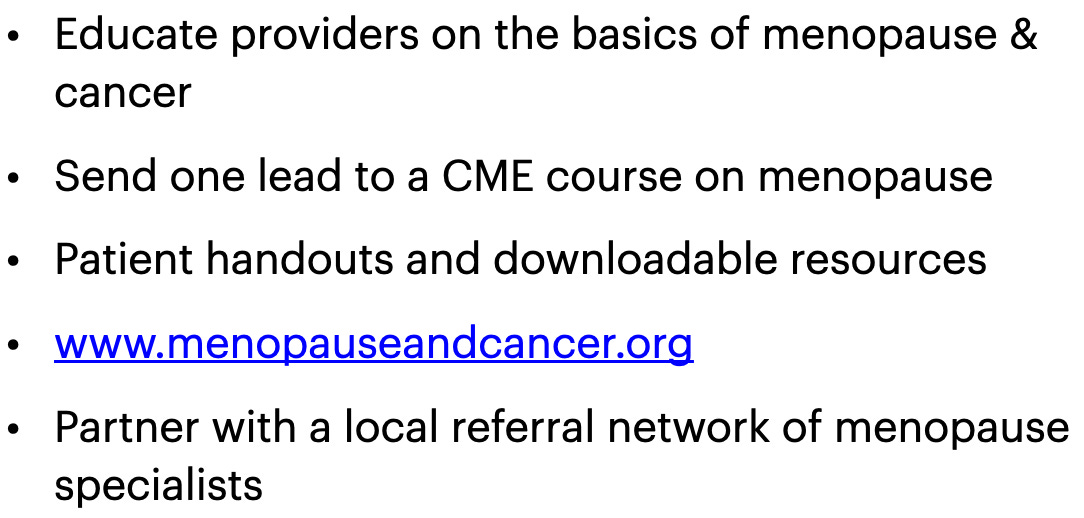
Did you know that superman was created in Cleveland? Here is what I told the audiene about how to be a survivorship superhero!
During my GSM presentation, I showed a room full of medical oncologists, surgeons, nurses, and navigators slides of breast cancer treatment induced GSM photos, because we must face and describe accurately what GSM actually is - and how devastating it can be when left untreated. I bet that was the first time the NCoBC had photos of clitoral adhesions on the main stage! I reminded them that COOKING OIL IS NOT EVIDENCE-BASED MEDICINE FOR GSM! The tide is turning and hopefully more patients will get access to vaginal hormones.
This quote perfectly states how I believe we must practice. “Ultimately, however, women with breast cancer should be treated as partners in their own care. They deserve an accounting of what is known, what is uncertain, what is feared, what evidence we have, and what options and trials exist—so they can weigh possible cancer-related risks against daily symptom burden and other competing health risks. When uncertainty is high, shared decision making and careful follow-up are not extras; they are the core of high-quality care.”
They go on with a Call To Action:
”We call on oncologists and professional societies—ASCO, American College of Obstetricians and Gynecologists (ACOG), and others—to re-evaluate the hormone therapy literature and allow for nuanced considerations of the data that encourage individualized approaches. We congratulate the recent Menopause Society multidisciplinary panel calling for shared decision making and clinical trials for MHT in women with breast cancer and the 2026 JAMA viewpoint by Pleasant and Ring who emphasized that, in the face of the literature we have, despite uncertainties, personalized shared decision making and expanded clinical trials are our way forward.”
”In conclusion, we believe that clinicians should acknowledge that the data associating MHT and breast cancer recurrence are not definitive and that addressing treatment-related menopause symptoms is as important as optimizing adjuvant therapy to improve health. While we appreciate that ASCO plays an important role in guiding quality oncology care, the data support reconsideration of its stance on MHT after breast cancer, including for those with hormone-positive disease. Our survivorship approach must reflect a personalized framework that explains the data more accurately—including its strengths and weaknesses—and leaves room for patients to make their own decisions.”
So that’s a wrap of my March happenings! Next up- on Monday I am giving virtual Grand Rounds at Weill Cornell Genetics and Personalized Cancer Prevention Program (GPCP)! They want to learn more about how to support their high-risk patients and BRCA carriers!
The menopause movement is trickling down to the most vulnerable and left-out women, slowly but surely. We have a lot of work to do and a lot of doctors and patients to educate, but I am optimistic. So I will leave you with the lyrics of the hype song I had playing in my headphones before I took the stage at the Harvard, along with a picture of the beautiful ballroom ceiling where the conference was held.
”And that's when I told you It's alright You were dancing through the lightning strikes Sleepless in the onyx night But now the sky is opalite.”
This Substack is reader-supported. To receive new posts and support my work, consider becoming a free or paid subscriber.
Glynne S, Simon J, Branson A, Payne S, Newson L, Manyonda I, Cleator S, Douek M, Usiskin S, Tobias JS, Vaidya JS. Menopausal hormone therapy for breast cancer patients: what is the current evidence? Menopause. 2026 Jan 1;33(1):88-117. doi: 10.1097/GME.0000000000002627. PMID: 41025376; PMCID: PMC12727074.
Pleasant V, Ring K. What Systemic Hormone Therapy Black Box Removal Means for Breast Cancer Survivors. JAMA. 2026 Mar 3;335(9):749-750. doi: 10.1001/jama.2026.0025. PMID: 41642590; PMCID: PMC13061421
Thanks for your tireless work on this! We are working to improve this care at my institution and it’s helpful to keep up to date on all the latest papers and meetings. Excited to read this new paper in the oncology journal. Some of the push back I have heard is all the info is coming from TMS and ACOG. Thanks for helping make it easier to keep up :)






Thanks for your tireless work on this! We are working to improve this care at my institution and it’s helpful to keep up to date on all the latest papers and meetings. Excited to read this new paper in the oncology journal. Some of the push back I have heard is all the info is coming from TMS and ACOG. Thanks for helping make it easier to keep up :)